Business
Bengal Violence: The Difficult Reality Of Becoming A Doctor In India
- For many families in India a career as a doctor is much sought after. But what does it entail? Are those that opt for such a career going in with their eyes wide open?
- And is it fair that after all such hard work to become a doctor, they have to face irate mobs that pose a threat to their lives?
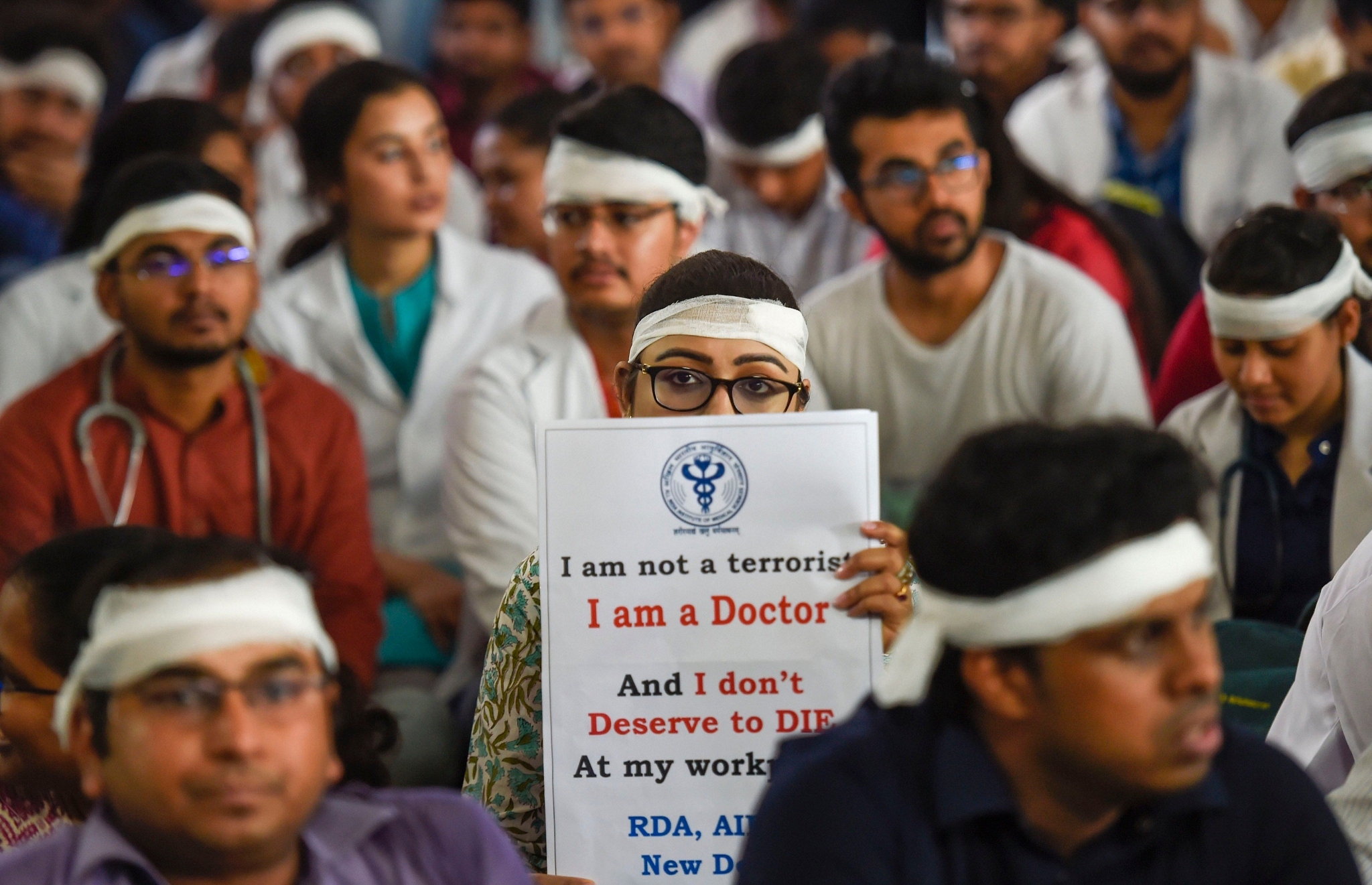
Doctor’s protesting Source: Twitter (NDTV)
It took the fractured skull of a junior doctor, Paribaha Mukhopadhyay, for a nation of over 1.3 billion people to realise the routinely prevailing violence against doctors in India. Nil Ratan Sircar Medical College and Hospital, or the NRS hospital, witnessed violence of an unprecedented scale after Mohammed Sayeed, aged 75, passed away. He was undergoing treatment at the hospital.
The family alleged medical negligence on the part of the hospital, and on the evening of the death, a mob of more than 200 people attacked the hospital. Speaking to one of the witnesses to the attack, Swarajya learned that the patient’s family had put the blame of Sayeed’s death on the doctors, alleging that the doctors had killed Sayeed with an injection.
Before the frenzied mob, the police outside the hospital was helpless. The mob unleashed its fury on the doctors and interns working in the NRS hospital and left, leaving behind a carnage that served as a wakeup call for doctors and citizens across the country.
However, this was not the first time doctors or interns had been attacked by a patient’s friends or relatives in NRS hospital, or in Kolkata, or West Bengal, or anywhere else in India. What troubled the doctors this time was not the attack, but the audacity that inspired it, the evident brutality, and their own increasing vulnerability before an unpredictable fanatical mob.
For an electorate that found itself obsessed with the idea of ‘roti kapda aur makaan’ across the first five decades of independence, the healthcare infrastructure was not that big a priority.
Yet, in 2019, we have come a long way from an overall life expectancy of 32 years, an infant mortality rate (IMR) of 146/1000 live births, a maternal mortality ratio (MMR) of 2000/100,000 live births, 50,000 odd doctors, and only a little more than 700 primary healthcare centres (PHCs) in 1947.
In terms of MMR, we now stand at 174 for every 100,000 live births, even though Thailand, China, and Sri Lanka have an MMR of 20, 27, and 30 respectively. India’s IMR has come down to 38/1000 live birth, though higher than the IMR of Sri Lanka, Nepal, Thailand, and even Bangladesh.
Even if one accounts for the giant strides taken to counter the MMR and IMR, there is the issue of a rising patient count for other diseases.
For instance, when it comes to tuberculosis (TB), India tops the global rankings, with over 2.7 million cases in 2015 alone. An underlying current of non-communicable diseases has swept through urban India with a higher number of cases under diabetes, cardiac arrest, clinical depression, amongst others being registered. To make matters worse, we have the curse of land, air, and water pollution.
Even with all the cleanliness drives, toilets, LPG cylinders, and Jan Dhan bank accounts, the development of rural India shall boil down to the government’s investments in the healthcare sector. These investments must go beyond physical infrastructure and get into human resources, for this is where the biggest challenge in the healthcare sector lies.
For a majority of middle-class parents in India, a career in medicine or engineering for their wards is the ideal way of life.
Today, there is an oversupply of engineering seats and engineers with a lack of employable skills across sectors. Many unemployed engineering graduates turn to a career in management for better job prospects. For the students of medicine, the story is starkly different, and difficult.
The journey for any aspirant begins at the age of 15-16, right after they complete their matriculation. Across Class 11th and 12th, the aspirants are required to enrol themselves into coaching centres that offer to tutor for NEET (National Eligibility cum Entrance Test). The fee alone for these coaching centres kills the dream of many aspirants from the lower economic strata of society. This is the first stage where millions in India give up on their dream of becoming a doctor.
For the ones who are fortunate enough to have their parents sponsor the fee for NEET coaching, the next two years warrant long studying hours. The duration of a coaching class ranges between six to twelve hours, leaving the remaining hours of the day for self-study and sleep, if one can afford it.
For many, at the age of 15 and 16, the stress is too much to handle. Often, it has been seen that aspirants make a shift from PCB (physics, chemistry, and biology) to PCM (replacing biology with mathematics) within the first three to six months of their coaching. This is because the probability of getting into a government engineering college is far greater than that of getting admission in a government-run medical institution. This is the second stage where the field sees many dropouts.
The NEET is a different ball game altogether. Success in the first go is rare. Also, the prevailing reservations make it difficult for everyone to get through, even the intelligent ones. Thus, many turn to a career in pharmacy, teaching, and even commerce or arts. This is stage three when it comes to students giving up on their ambitions in medicine. Some, however, keep trying for the exam for two to three years after their Class-12 exams.
For the ones who manage a seat in one of the government colleges, or even private ones with the help of generous sponsors or hefty donations, reality kicks in. In the first year of MBBS (Bachelor of Medicine and Bachelor of Surgery), an undergraduate course that runs for five-and-a-half years, the students struggle with the long hours, with aligning themselves with the exam and class routines, and often, with the subjects.
It is not uncommon for students to fail in the first year of their MBBS’ regular exams, take the NEET again, and start their MBBS all over again. Some choose to quit MBBS altogether. There have been cases where students opted out of MBBS because they were not emotionally comfortable with body dissection, a foundational activity in the field of medicine and surgery. This is the fourth stage when dropouts occur.
For the ones who move to their second year, life becomes increasingly difficult. As they watch their engineering peers get into internships and a relatively easy way of life, the students in medicine find themselves engrossed in elaborate subjects. Another difficulty at this stage is that most books are authored by experts from the West. Thus, it warrants a lot of catching up for those students who have not studied with English as their first language in school, or for those who come from rural regions.
In one of its conversations, Swarajya learned how students often give up on their ambitions in the second year as well. For some students, performing an autopsy is when they call off their relationship with medicine. The doctor in conversation with Swarajya, narrated how she puked before the very body she was required to perform an autopsy of. However, she continued with her MBBS, as many students do.
By the end of the second year, the stress kicks in. Many start feeling depressed, for the long hours, tedious lessons, and lack of work-life balance leave no room for a social life. Students find themselves estranged from the very social circles that were once indispensable to their lives. This is the last instance, or stage five, where a few choose to give up on MBBS and turn to a relatively easier career choice.
The 3rd and 4th years, as Swarajya learned in its interaction with the doctors, are relatively easy, as by now, the students have aligned with the needs of the course. Though subjects are easy or difficult, based on personal interpretation, this is a critical year for it forms a bridge between theoretical learning and practical implementation.
By the end of the 4th year, the students find themselves working with their seniors and other doctors on real-life cases. The practical learning in this phase is something that cannot be found in books or online lectures. While the syllabus is vast and encompasses a wide area of medicine and surgery, this is the phase that begins the process of moulding students into doctors.
The remaining year-and-a-half is spent across all departments. However, for most undergraduates, this period comes with severe peer pressure for they find their friends settled with high-paying jobs while they stand before another mountain to climb, that of post-graduation.
Speaking to Swarajya, a doctor recalled her final months of MBBS, “In the final year of MBBS, one is exposed to many areas of surgery and medicine, but that is like being a jack of many trades without being a master in any, and this is where the post-graduate courses come into play.”
This threshold between MBBS and an uncertain NEET-PG entrance is when stage six comes into play. A lot of students, upon not being able to clear the NEET for post-graduate courses, opt for alternate careers. Some turn to India’s most sought-after jobs by clearing the UPSC, and some opt for teaching. However, at 23 or 24, many invest another two or three years of their lives to crack the entrances for post-graduation (PG).
A lot of students, upon not going through NEET-PG in the first two instance, migrate abroad. For the ones under tremendous financial stress, or an inability to afford the excruciating high fee in the absence of a top rank, an alternate career is inevitable, and this is how the field sees a lot of dropouts at this stage.
Thus, if resilient, at the age of 24-25, the students of medicine find themselves before a three-year specialty course, either in medicine or in surgery. Also, the post-graduate course comes with a minimum stipend.
The sailing, however, gets rougher from here, for now, even longer working hours come into play. Doctors, especially the ones pursuing a specialty in surgery, for instance, gynecology, are on-call or on active duty anywhere between 12 to 60 hours. One of the doctors, in conversation with Swarajya, narrated how a 60-hour call was routine for her in the second year of her MS (Master of Surgery).
While quitting is no longer an option for MD and MS students, they find themselves fighting personal battles with their seniors. Harassment over personal issues, public insults, agreeing to personal favours, bribing examiners, and even paying for their seniors’ fuel and shopping is a common practice amongst students pursuing PG. Recently, a 26-year old doctor in Mumbai, pursuing MS in gynecology, committed suicide, for she was harassed by her seniors over her caste.
“What she felt, a lot of us feel, for different reasons,” a doctor narrates. “Unfortunately, she couldn’t take it anymore. Often, we feel the same way. I once wanted to jump from the terrace of the hospital, and that’s when I rang my mother who is also a doctor. This is how most of us feel, but we have to keep going, for ourselves, for the investment we have made, and for our families,” she tells Swarajya. “Given there are not enough doctors for the patients, we are left with no time for research”.
As it turns out, apart from all of this, there is yet another frontier where doctors have to fight battles every other day.
Narrating a common cause of the patient relatives and doctor conflict in one of the government hospitals of Aurangabad, a doctor tells Swarajya about how once every week or two, someone tries to incite violence against the doctors. This story comes from a gynaecologist.
“Often, we have people from a certain religious community who are against the delivery of a baby via the method of Caesarean section, also known as C-section. They force us to have the delivery the natural way, citing their religious practices,” she tells Swarajya. “As doctors, we take into account the safety of the mother and the child, and that is all that matters to us, but we often find ourselves in conflict with the parties representing the women. They want us to perform a natural delivery, even if it means the death of the child, only because they want to ensure that their wives go on to have 6-8 children, irrespective of their poverty.”
The doctors, in conversation with Swarajya also narrated instances where resident doctors, interns, and newly-admitted PG students had to rush to their rooms, fearing violence from the patients’ family. “We are not Gods, nor we claim to be, but if we suggest an alternate method of treatment, they blame us saying that we are doing so to increase the medical bill. It is so difficult to knock sense into some of the patients’ families. If we suggest a better treatment, we are cronies, and if we fail in saving one of their own, we are murderers,” they say.
Clearly, what happened in Bengal was not the first or last case of violence against the doctors by patients’ families or friends. Today, doctors in India find themselves traumatised by the mob violence that found an indirect encouragement from the West Bengal Chief Minister.
“Even when we were on a strike, we were all in the emergency ward. We cannot let anyone die on our watch. While the strike had the normal wards closed, the emergency wars were fully operational”, a doctor from Kolkata told Swarajya.
It turns out that doctors across the country, even during the strike on 17 June, were working in emergency wards, looking after patients who required urgent attention. “I finished three successful deliveries on Monday,” the doctor from Aurangabad tells Swarajya, “and all this while female resident doctors and interns in West Bengal were fearing acid attacks and rape.”
Being a doctor in India amounts to a psychological battle that is to be won each day. For the ones who are brave, intelligent, and resilient enough to overcome a decade of studies that encompass preparation for entrances, MBBS, and MS or MD, the challenges in the professional realm are many.
There is stress, for the limited workforce and long working hours are non-negotiable. Then comes the guilt for even the most brilliant medical minds will have patients that are beyond saving.
Now, to add to the stress and guilt, there is also the ever-increasing fear of mob violence, similar to what was seen at the NRS hospital.
“I once came out of the operation theatre after a failed delivery. The child was dead, and as I stepped out of the room, I was greeted by another man, who had become a father an hour ago, with sweets. I obliged, congratulated him, and moved on to another patient,” a doctor recalls. “That is what goes on every day, a never-ending show.”
This show is indispensable to India’s and perhaps the world’s biggest healthcare project, Ayushman Bharat. Merely enabling access for 500 million people is not going to suffice, for the government needs to invest in getting more hands on the deck.
Today, any emergency in a government hospital finds a couple of doctors swamped by over 30 patients’ families. In addition to this, there are long working hours, lack of infrastructural support in many rural districts, and the lack of beds for the general population. A trip outside AIIMS in New Delhi on a cold winter night would lead to one witnessing people sleeping outside in the cold while undergoing treatment during the day. This occurs in many other government hospitals across India. There are just not enough beds to accommodate the never-ending stream of patients nor are there enough doctors to attend to this huge inflow of patients.
India needs more doctors, the ones who can go through a decade of hard work, resilience, and the harsh reality that accompanies the educational system in India. Today, while these heroes find themselves under attack from rogue mobs, their only hope lies with the central government.
In return, the latter must step up, given that the quest for a $6 trillion economy will not be complete without a thriving healthcare setup that encompasses infrastructure, human workforce, research, development, and innovation. Having innovation labs under different missions won’t be enough if we do not give the best minds of this country enough time for research.
The government’s role in providing security for doctors is non-negotiable. There is no ease of anything, business or living, when a nation’s doctors are under attack, or under the fear of one. Today, the fractured skull of a junior doctor from West Bengal mirrors the fractured healthcare system of the country as a whole.
Doctors are not Gods, and people must not forget that despite their heroics and faults, they are humans too.
Support Swarajya's 50 Ground Reports Project & Sponsor A Story
Every general election Swarajya does a 50 ground reports project.
Aimed only at serious readers and those who appreciate the nuances of political undercurrents, the project provides a sense of India's electoral landscape. As you know, these reports are produced after considerable investment of travel, time and effort on the ground.
This time too we've kicked off the project in style and have covered over 30 constituencies already. If you're someone who appreciates such work and have enjoyed our coverage please consider sponsoring a ground report for just Rs 2999 to Rs 19,999 - it goes a long way in helping us produce more quality reportage.
You can also back this project by becoming a subscriber for as little as Rs 999 - so do click on this links and choose a plan that suits you and back us.
Click below to contribute.
Latest