Ideas
Vaccine Rollout In A Pandemic: Why Prioritised Access Drives Public Policy
- India has kept pace with efficient public policy responses across the world — demonstrating the ability to independently develop vaccines and produce at scale.
Covaxin Covid-19 vaccine (Pic Via Twitter)
In recent days, we have seen a spirited debate on whether vaccinations should or should not be opened up to all, and let ‘the market work’ by enabling people to pay the prices they can.
The government argues against this and Dr Harsh Vardhan, Union Minister for Health and Family Welfare, had to issue an unprecedented press release with data explaining why a free for all was premature. This article sheds light on the issue.
Public Policy Response To Covid-19: Vaccine Development
Covid-19 has presented a once in a lifetime public policy and public health management challenge to every government across the world. The world has not seen such a pandemic in a century, since the 1918 Spanish Flu pandemic, which killed 13-18 million Indians, a figure that is multiples of the mortality in the Bengal Famine in the middle of the Second World War.
India has been relatively fortunate in that it has been able to keep up with the best of public policy responses across the world — demonstrating the ability to independently develop vaccines (eg, Covaxin and others) and the ability to produce at scale as Serum Institute of India (SII) has done with Covishield.
There are a large number of countries — even advanced ones — with no local vaccine candidate in advanced trials, and with no local manufacturing base who are struggling to get hold of supplies at all. There are ongoing vaccine fights — [read here, here, and here — over various related causes.
The Indian government has steered public policy response in a manner that largely protected India from having to struggle against such factors outside of our control, in terms of access to the basic science, technology and production facilities associated with vaccine development. Most others lack in some or all of these.
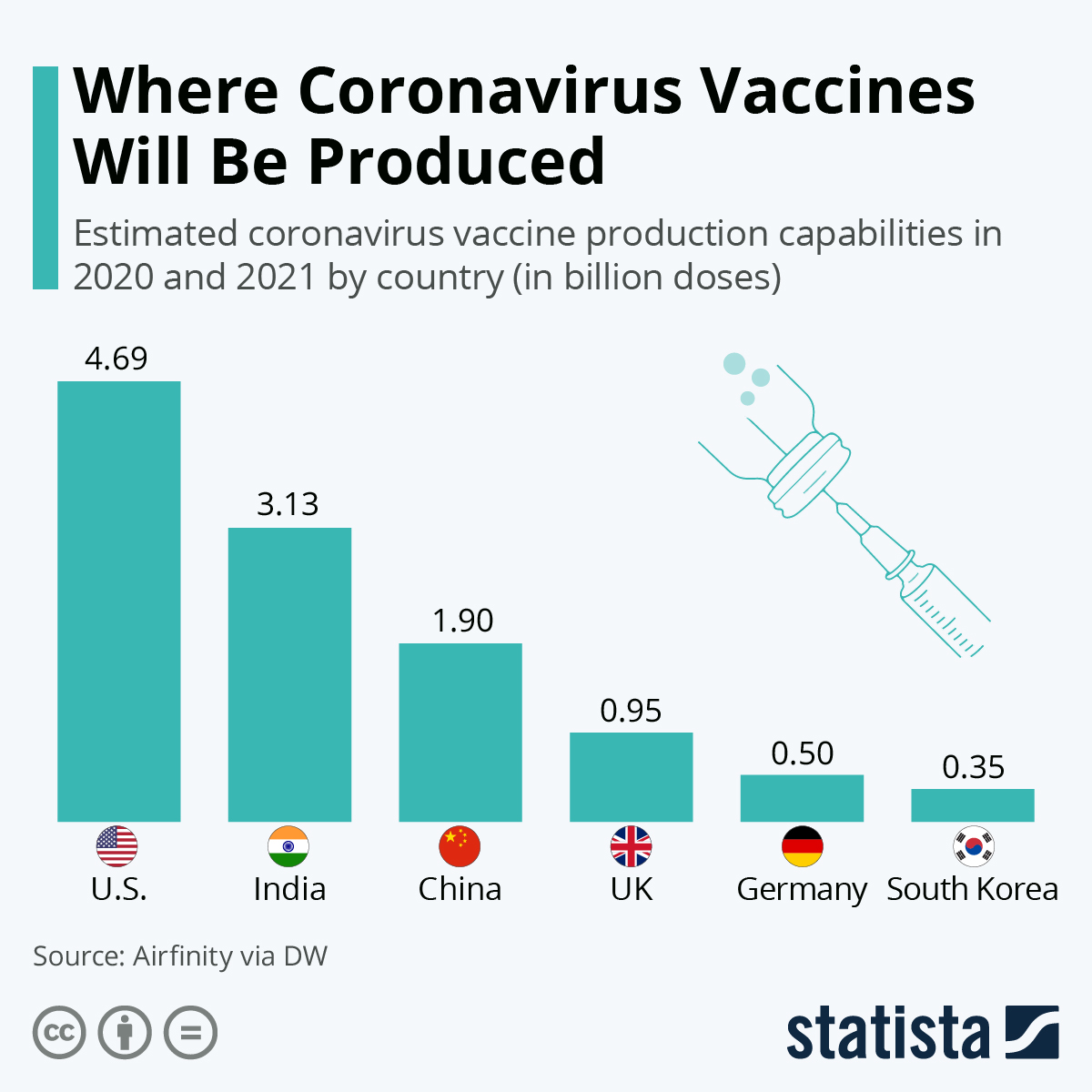
Only four countries in the world today have so far shown independent capability to develop and mass produce Covid vaccines — India, China, the US and Russia. Only the first three have capability to produce multiple billions of doses a year. While other countries with multinational big pharma operations have played important roles, these four are the only ones who have shown the ability to develop, produce and distribute at scale.
{kind=link}
All current Covid vaccines are being distributed under emergency use authorisation (EUA) — the accelerated mechanism by which vaccines are being rushed to use. Typical vaccine development takes up to 10 years. Due to the nature of the pandemic, the process was dramatically accelerated worldwide.
The accelerated approval processes have caused controversy: Covaxin received EUA under restricted clinical trial mode while still in phase 2/3 trials and this was depicted as hasty. However, they completed phase 3 and submitted results to The Lancet.
However, this is not unprecedented. The Pfizer/BioNTech vaccine also got early EUA on 18 November 2020 while FDA was reviewing its data, a subsequent EUA on 11 December 2020, and a further revision in late February 2021. While not ideal, this is the Covid ‘new normal’.
Public Policy Response To Covid-19: Vaccine Production
Typically, the world consumes around 1 billion doses of vaccines a year. Covid has caused an order of magnitude increase in demand, requiring two doses per head for most of the world, or about 16 billion doses.
The Indian Council of Medical Research (ICMR) maintains information on the status of every Covid-19 vaccine trial in India. Only Covaxin and Covishield have received Drug Controller General of India (DGCI) approval after completing phase 3 trials. Both are in production in India today.
The SII is the world’s largest vaccine maker. It produces the Oxford/Astra Zeneca vaccine under the brand name Covishield. It has a current monthly production capacity of 60 million per month, to increase to 100 million a month in May. The SII is a manufacturer and not an R&D establishment. Bharat Biotech, which developed Covaxin, lacks the SII’s production scale. Both have requested funding — SII requested Rs 3,000 crore ($403 million) to build more production capacity, while Bharat Biotech is scaling up from its current 4-10 million a month to 7x that figure. US vaccine production received billions from their government.
Despite restricting vaccinations to those over 45, India currently vaccinates over 3 million a day, accelerating at the same rate as China recently and much faster than any other country on the planet. Indian cumulative vaccination count exceeds the combined EU and is behind only US and China:
That extrapolates to about 80 million vaccinations a month assuming the current drop on Sundays — at the very upper end of the combined total production capacities of both Covishield and Covaxin.
India currently vaccinates an Australia worth of people a week, despite only those above 45 permitted. Four million vaccinations/day requires over 110 million vaccines a month. Five million/day requires 14-150 million/month production.
Large scale vaccine production is hard. Even the US asks itself "with billions spent and wartime status, why are vaccines in short supply?". Given these circumstances, India is a peer of the two largest manufacturing entities in the world — the USA and China — despite being a fraction of the size of those two economies.
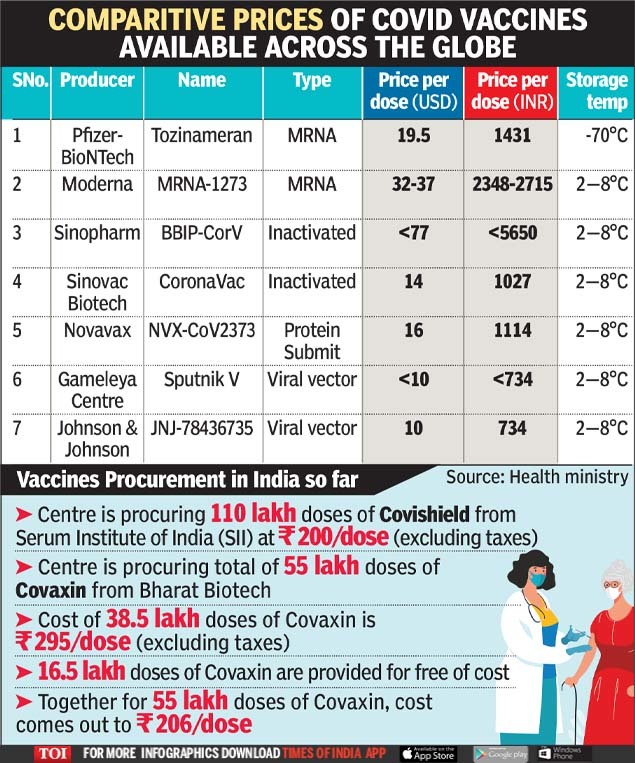
In addition, the Indian government has the most competitive procurement costs in the world for Covid-19 vaccines, with other countries paying up to 10x per dose compared to what the Indian government obtains and makes available these vaccines for.
{kind=link}
Public Policy Response To Covid-19: Vaccine Prioritisation
The ICMR and MoHFW have published an excellent Covid-19 communication strategy document in 2020. It describes a plan of communicating vaccine availability, mobilising vaccination plans, the use of government, media, religious leaders and civil society to drive vaccination. In page 64, it outlines the recommendations for vaccine prioritisation.
The ICMR’s priority recommendation mirror those made by ACIP of the CDC for US, the PHE recommendations in UK, and the German priority groups. Indian Priority group 2 (60 and over, 45 and over with comorbidities) began on 1 March and group 3 (all 45 and over) began on 1 April. The US is currently in phase 1B/1C in most major areas. In effect, both countries are vaccinating the same priority group right now.
Why not just make the vaccine available freely?
As we have seen, production is still scaling up, and therefore free market supply and demand considerations are not the driver. Further, ‘demand’ in this case must be quantified. Who needs vaccines the most? The ICMR communication strategy document lists two priorities (page 64):
a) Those at the greatest risk of exposure to infection and age group having high Covid related death.
b) Those when vaccinated would minimise the spread of the virus.
The Lancet published data reporting Covid-19 mortality risk by age group:
Current Indian vaccination priority is exactly aligned to the data above — it targets the more than 45 age group who are at least 10 times more at risk than those younger. Someone in their 80s faces an almost 50 per cent chance of dying if they get Covid-19. Effective public health policy must target the safety of the most vulnerable groups first — and it currently does so.
The second priority of vaccination is to target those most likely to spread. To accomplish this, the government has scaled up vaccination and announced that vaccines will be available seven days a week at public and private vaccine centres. From 11 April, vaccination camps are being organised at workplaces for employees aged 45 and older. The same facilities can be expanded with no overhead as the eligibility group is widened.
The population pyramid of India shows that 10 per cent of the population is over 60. Under 25 per cent of the population are in the over 45 group. The latest vaccination data as of 7 April shows that almost 59 million people across the 45-60 and 60+ age groups have received at least one dose of vaccine.
At the current 3 million/day, by the end of April India will have given a first dose to 120-130 million or around 45 per cent of the population most at risk — within this month. By doing so we will see the results seen in Israel, where high vaccination coverage among the high risk group dramatically lowered mortality figures.
While the virus will continue to propagate, public health policy dictates that the best approach to saving lives is to target vaccination of the groups most at risk.
The ICMR communication document makes a strong case for a concerted national effort supporting the vaccination programme. By any measure, India has so far been amongst the best performing countries in the world. It has independently developed a vaccine, has acted as a major production and export node, and has — in the face of criticism — applied good science to target the most high risk groups, and has done so at a pace as good as the best in the world.
Support Swarajya's 50 Ground Reports Project & Sponsor A Story
Every general election Swarajya does a 50 ground reports project.
Aimed only at serious readers and those who appreciate the nuances of political undercurrents, the project provides a sense of India's electoral landscape. As you know, these reports are produced after considerable investment of travel, time and effort on the ground.
This time too we've kicked off the project in style and have covered over 30 constituencies already. If you're someone who appreciates such work and have enjoyed our coverage please consider sponsoring a ground report for just Rs 2999 to Rs 19,999 - it goes a long way in helping us produce more quality reportage.
You can also back this project by becoming a subscriber for as little as Rs 999 - so do click on this links and choose a plan that suits you and back us.
Click below to contribute.
Latest